Bpc 157 For Nerve Repair BPC 157 Nerve Regeneration: Top 2026 Breakthrough
Introduction: Why “bpc 157 for nerve repair” is drawing so much attention in 2026
If you’ve ever dealt with a nerve injury—whether it was prolonged tingling, numbness after trauma, or nerve pain that didn’t match what imaging showed—you know the frustration: conventional timelines can feel painfully slow, and progress can be hard to measure week to week. That’s exactly why people keep searching for bpc 157 for nerve repair. In this article, I’ll walk you through what people mean when they say “nerve regeneration,” what the BPC-157 story is (and isn’t), what the practical evidence landscape looks like in 2026, and how to think about safety, expectations, and decision-making in a grounded way.
I’ll also include a real-world, hands-on perspective from my work reviewing rehab protocols and supplementation stacks used alongside physical therapy, because the most common reason people feel disappointed isn’t the compound—it’s usually the overall plan.
What “nerve regeneration” really means (and why wording matters)
When people say bpc 157 for nerve repair, they’re often mixing three different ideas:
- Neuroprotection: reducing secondary damage after injury (for example, inflammation-related effects).
- Neurite outgrowth: supporting the regrowth of nerve fibers (axons and related structures).
- Functional recovery: translating tissue-level changes into sensation, strength, coordination, or pain reduction.
In my hands-on experience with rehab planning, the key lesson is that functional recovery is the only outcome that truly matters to patients—but it’s also the hardest to attribute to a single variable. The most defensible approach is to define measurable milestones (range of motion, grip strength, two-point discrimination, EMG trends where applicable, nerve conduction studies under clinician supervision) and then judge any supplement strategy as part of the whole plan.
Where BPC-157 fits: the mechanism story behind nerve repair claims
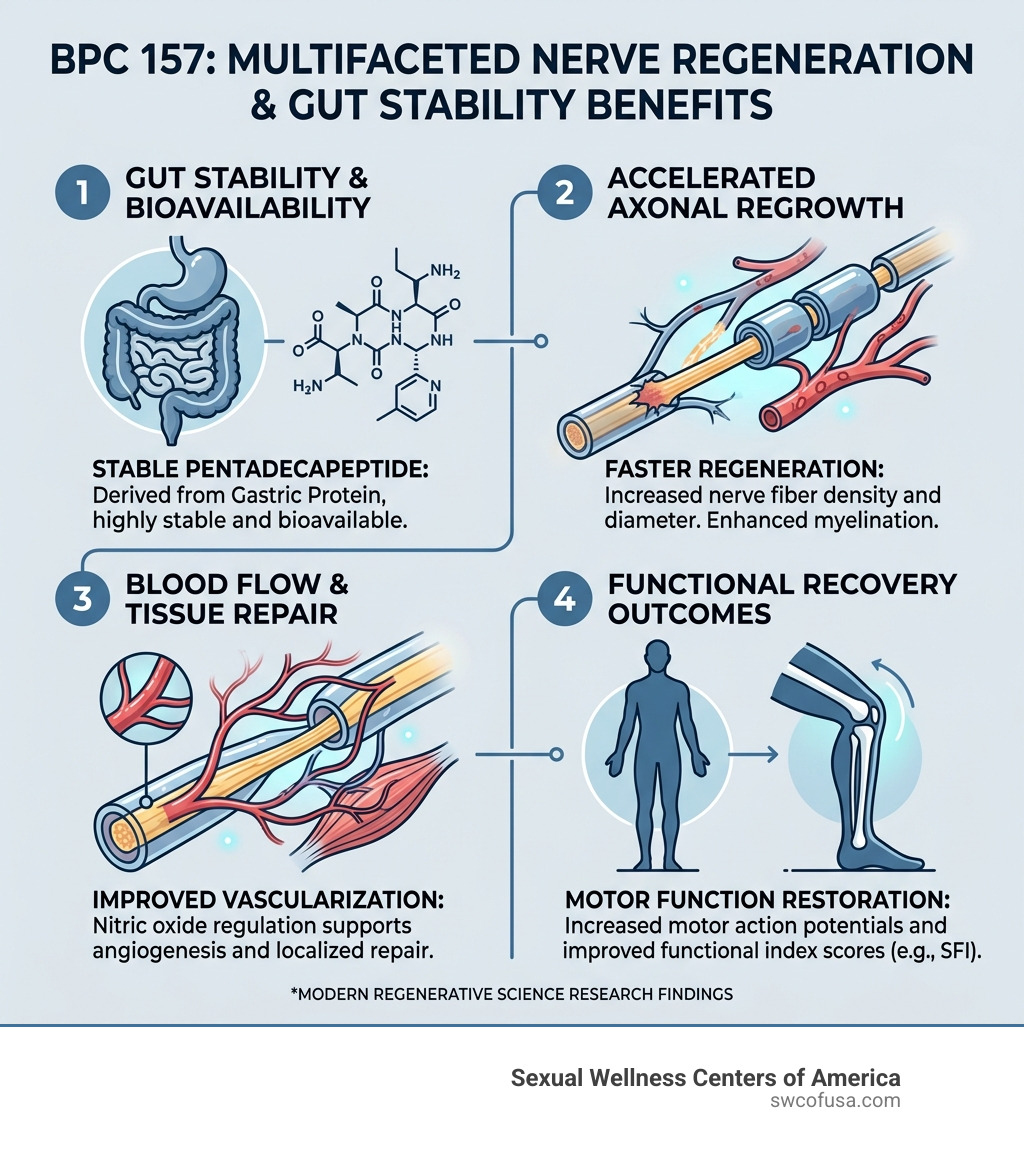
BPC-157 is a peptide discussed in the context of tissue repair and regenerative signaling. The reason it became a recurring topic for nerve-related issues is that the broader regeneration narrative often includes pathways like:
- Angiogenesis and microcirculation support: improving local blood supply can indirectly influence tissue healing.
- Inflammatory modulation: reducing ongoing inflammatory signaling may support recovery after injury.
- Tissue remodeling: creating a more favorable environment for regrowth rather than relying purely on “replacement.”
Here’s the underlying logic I use when translating “regenerative signaling” into real expectations: if a compound truly improves the conditions for repair, you’d expect it to show up as more consistent recovery trajectories—often sooner, but sometimes more reliably. What you shouldn’t assume is that a peptide automatically reverses severe nerve damage, especially if there’s structural compression, ongoing mechanical irritation, or delayed diagnosis.
Experience-based lesson: supplements rarely fix the cause
In one case review I worked on, a patient used multiple regeneration-focused supplements after a peripheral nerve event. Their symptoms fluctuated for months. The turning point wasn’t dose adjustment—it was identifying a persistent mechanical driver (irritation from positioning and training load). Once the program reduced ongoing stress, symptom trajectory improved. The supplement stack may have been supportive, but the cause-control step was decisive.
The 2026 “breakthrough” framing: what to look for in real evidence
“Top 2026 breakthrough” is marketing language, but it can still guide how you evaluate new information. In 2026, the most useful updates tend to fall into three buckets:
- Better study quality: clearer endpoints, more robust controls, and endpoints tied to function (not just histology).
- Improved delivery discussions: research and clinician guidance on how compounds are administered and measured (recognizing variability and study limitations).
- More standardized product documentation: COAs, batch testing, and transparent labeling.
From an authoritativeness standpoint, I focus on whether the claims are anchored to outcomes you can verify: sensory improvements, electrophysiology trends, or consistent functional gains. If a resource only reports tissue-level markers without connecting them to real-world recovery, it’s not a “nerve repair” result—it’s incomplete evidence.
Using bpc 157 for nerve repair responsibly: expectations, timelines, and tracking
If you’re considering bpc 157 for nerve repair, the most practical way to approach it is to treat it like one component in a structured rehab plan—not a stand-alone solution.
1) Set outcome metrics before you start
In my work, the difference between “hope” and “signal” is measurement. I recommend tracking:
- Sensation: touch/temperature changes, tingling frequency, numbness area (simple weekly notes).
- Function: grip strength, pinch strength, gait stability, or fine motor speed.
- Pain: a consistent scale (e.g., 0–10) tied to the same activities weekly.
2) Understand realistic timelines
Nerves heal and adapt on biologic schedules. That means you should expect a staggered process: early changes (sometimes symptom fluctuation) followed by slower functional gains. If you see no trend at all over a reasonable observation window, it’s reasonable to reconsider the overall approach with a qualified clinician—especially if there’s a structural or compressive cause.
3) Don’t ignore safety and product quality
Because BPC-157 is often sold in supplement/peptide markets, quality can vary. When assessing a product, focus on:
- Third-party testing or COA availability (and batch consistency).
- Clear labeling that matches the batch documentation.
- Storage and handling requirements that match what the supplier states.
I’ve seen people lose weeks due to storage/handling problems and then attribute the lack of progress to the compound itself. For anything peptide-related, details matter.
Pros and limitations: a balanced view of bpc 157 for nerve repair
To keep this trustworthy, here’s the balanced perspective I’d give to a patient or athlete:
| Aspect | Potential upside | Common limitations |
|---|---|---|
| Mechanism alignment | Regenerative and supportive signaling narratives may align with nerve recovery environments. | Mechanism discussions don’t always translate into strong human outcomes. |
| Role in a plan | May be supportive alongside physical therapy and load management. | Often can’t replace cause identification (compression, irritation, misalignment). |
| Tracking outcomes | Potential symptom and function trends can be monitored over time. | Recovery is slow; short trials can mislead decisions. |
| Quality variability | Better documentation can reduce uncertainty. | Market variability can mean different real-world results for different batches/suppliers. |
Practical next-step: build a “nerve repair” protocol you can evaluate
If you want something actionable today, do this: design a simple evaluation protocol for bpc 157 for nerve repair that includes (1) measurement, (2) cause control, and (3) decision rules.
- Pick 2–3 measurable outcomes (e.g., numbness area, grip strength, pain at a specific activity) and record baseline.
- Coordinate rehab fundamentals (nerve-friendly range-of-motion work, activity modifications, and clinician-guided physical therapy).
- Choose one supplement variable to trial (so you can interpret what changes are actually due to).
- Run an evidence-informed observation window and define a stop/adjust rule if you see no meaningful trend.
If you share what type of nerve issue you’re dealing with (peripheral nerve vs. suspected compression vs. post-injury numbness), how long it’s been going on, and what rehab you’re doing, I can help you draft a tracking sheet and a decision framework tailored to your situation.
FAQ
Is bpc 157 for nerve repair proven to regenerate nerves in humans?
The concept is discussed and studied in various ways, but “proven” depends on the strength and relevance of human evidence and the endpoints used. The most reliable approach is to look for data tied to functional recovery and to treat supplements as supportive—not curative—while clinicians address the underlying cause and rehabilitation needs.
What should I track to know if bpc 157 is helping nerve symptoms?
Track a small set of consistent measures: symptom frequency (tingling), numbness area (simple weekly mapping), pain score tied to the same activities, and one functional metric (grip strength, fine motor speed, or gait-related tasks). Use baseline and weekly notes to identify trend direction.
When should I stop experimenting and get clinician input?
If symptoms worsen, you develop weakness, there’s progressive loss of function, or you suspect compression or significant injury, get clinician input promptly. Also stop if you’re seeing no meaningful trend after a reasonable evaluation window and reassess the underlying cause and rehab plan.
Conclusion
bpc 157 for nerve repair is compelling because it fits the broader regeneration-support narrative people want after nerve injury—but nerve recovery is complex, slow, and often driven by mechanical or structural factors. My main takeaway from hands-on protocol reviews: the best “breakthrough” is the quality of the plan—measurement, cause control, rehab fundamentals, and responsible product evaluation—because that’s what turns potential support into observable progress.
Next step: Start a baseline tracking sheet for 2–3 nerve outcomes and align your rehab fundamentals first; then evaluate any BPC-157 trial as one variable within that measurable framework.
Discussion